Bursitis Of The Heel Indications
Overview
Between the heel bone and the plantar fascia is a small fluid filled sac that is called the plantar (bottom of) calcaneal (heel bone) bursa. The plantar calcaneal bursa?s job is to allow the plantar fascia to glide easily over the heel bone without irritation. If this becomes inflamed and irritated a plantar calcaneal bursitis occurs which can be extremely painful and disabling forcing the athlete to stop training.
Causes
The most common causes of bursitis are injury or overuse, although infection may also be a cause. Bursitis is also associated with other causes, such as arthritis, gout, tendinitis, diabetes, and thyroid disease.
Symptoms
What are the symptoms of heel bursitis? pain, swelling, tenderness, redness, and/or warmth at either the bottom of the heel or top of the heel, depending on the degree of swelling, pain may be a dull ache or substantial enough to cause limping, running, jumping, and walking activities may exacerbate pain, wearing poorly fitting, tight, or high-heeled shoes may exacerbate pain.
Diagnosis
On physical examination, patients have tenderness at the site of the inflamed bursa. If the bursa is superficial, physical examination findings are significant for localized tenderness, warmth, edema, and erythema of the skin. Reduced active range of motion with preserved passive range of motion is suggestive of bursitis, but the differential diagnosis includes tendinitis and muscle injury. A decrease in both active and passive range of motion is more suggestive of other musculoskeletal disorders. In patients with chronic bursitis, the affected limb may show disuse atrophy and weakness. Tendons may also be weakened and tender.
Non Surgical Treatment
Podiatric Care may include using anti-inflammatory oral medications or an injection of medication and local anesthetic to reduce the swelling in the bursa. An injection may be used for both diagnosis and for treatment. When you go to your doctor, x-rays are usually required to evaluate the structure of your foot and ankle to ensure no other problems exist in this area. They may advise you on different shoewear or prescribe a custom made orthotic to try and control the foot structure especially if you have excessive pronation. Sometimes patients are sent to Physical Therapy for treatment as well. To aid in relief of pressure points, some simple padding techniques can be utilized. Most all patients respond to these conservative measures once the area of irritation is removed.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Between the heel bone and the plantar fascia is a small fluid filled sac that is called the plantar (bottom of) calcaneal (heel bone) bursa. The plantar calcaneal bursa?s job is to allow the plantar fascia to glide easily over the heel bone without irritation. If this becomes inflamed and irritated a plantar calcaneal bursitis occurs which can be extremely painful and disabling forcing the athlete to stop training.
Causes
The most common causes of bursitis are injury or overuse, although infection may also be a cause. Bursitis is also associated with other causes, such as arthritis, gout, tendinitis, diabetes, and thyroid disease.
Symptoms
What are the symptoms of heel bursitis? pain, swelling, tenderness, redness, and/or warmth at either the bottom of the heel or top of the heel, depending on the degree of swelling, pain may be a dull ache or substantial enough to cause limping, running, jumping, and walking activities may exacerbate pain, wearing poorly fitting, tight, or high-heeled shoes may exacerbate pain.
Diagnosis
On physical examination, patients have tenderness at the site of the inflamed bursa. If the bursa is superficial, physical examination findings are significant for localized tenderness, warmth, edema, and erythema of the skin. Reduced active range of motion with preserved passive range of motion is suggestive of bursitis, but the differential diagnosis includes tendinitis and muscle injury. A decrease in both active and passive range of motion is more suggestive of other musculoskeletal disorders. In patients with chronic bursitis, the affected limb may show disuse atrophy and weakness. Tendons may also be weakened and tender.
Non Surgical Treatment
Podiatric Care may include using anti-inflammatory oral medications or an injection of medication and local anesthetic to reduce the swelling in the bursa. An injection may be used for both diagnosis and for treatment. When you go to your doctor, x-rays are usually required to evaluate the structure of your foot and ankle to ensure no other problems exist in this area. They may advise you on different shoewear or prescribe a custom made orthotic to try and control the foot structure especially if you have excessive pronation. Sometimes patients are sent to Physical Therapy for treatment as well. To aid in relief of pressure points, some simple padding techniques can be utilized. Most all patients respond to these conservative measures once the area of irritation is removed.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Hammer Toe Pain Treatment Methods
 Overview
Overview
There are two different types. Flexible Hammer toe. These are less serious because they can be diagnosed and treated while still in the developmental stage. They are called flexible hammertoes because they are still moveable at the joint. Rigid Hammertoes. This variety is more developed and more serious than the flexible condition. Rigid hammertoes can be seen in patients with severe arthritis, for example, or in patients who wait too long to seek professional treatment. The tendons in a rigid hammertoe have become tight, and the joint misaligned and immobile, making surgery the usual course of treatment.
Causes
Hammertoe is caused when muscles fail to work in a balanced manner and the toe joints bend to form the hammertoe shape. If they remain in this position, the muscles and tendons supporting them tighten and stay that way. Causes of hammertoe can include squeezing into a too-small or ill-fitting shoe or wearing high heels that jam your toes into a tight toe box. An injury such as badly stubbing your toe. Arthritis. Nerve and muscle damage from diseases such as diabetes,
 Symptoms
Symptoms
A toe (usually the second digit, next to the big toe) bent at the middle joint and clenched into a painful, clawlike position. As the toe points downward, the middle joint may protrude upward. A toe with an end joint that curls under itself. Painful calluses or corns. Redness or a painful corn on top of the bent joint or at the tip of the affected toe, because of persistent rubbing against shoes Pain in the toes that interferes with walking, jogging, dancing, and other normal activities, possibly leading to gait changes.
Diagnosis
First push up on the bottom of the metatarsal head associated with the affected toe and see if the toe straightens out. If it does, then an orthotic could correct the problem, usually with a metatarsal pad. If the toe does not straighten out when the metatarsal head is pushed up, then that indicates that contracture in the capsule and ligaments (capsule contracts because the joint was in the wrong position for too long) of the MTP joint has set in and surgery is required. Orthotics are generally required post-surgically.
Non Surgical Treatment
If the toes are still mobile enough that they are able to stretch out and lay flat, the doctor will likely suggest a change of footwear. In addition, she may choose to treat the pain that may result from the condition. The doctor may prescribe pads to ease the pain of any corns and calluses, and medications ranging from ibuprofen to steroid injections for the inflammation and pain. Other options for non-surgical treatments include orthotic devices to help with the tendon and muscle imbalance or splinting to help realign the toe. Splinting devices come in a variety of shapes and sizes but the purpose of each is the same: to stretch the muscles and tendon and flatten the joint to remove the pain and pressure that comes from corns.
Surgical Treatment
In more advanced cases of hammer toe, or when the accompanying pain cannot be relieved by conservative treatment, surgery may be required. Different types of surgical procedures are performed to correct hammer toe, depending on the location and extent of the problem. Surgical treatment is generally effective for both flexible and fixed (rigid) forms of hammer toe. Recurrence following surgery may develop in persons with flexible hammer toe, particularly if they resume wearing poorly-fitted shoes after the deformity is corrected.
 Prevention
Prevention
Preventing foot problems, including hammertoes, is often a matter of wearing the right shoes and taking care of your feet. Check your feet regularly for problems. This is Hammer toe especially true if you have diabetes or any other medical condition that causes poor circulation or numbness in your toes. If you do, check feet daily so that problems can be caught early on.
How To Tell If I Have Overpronation Of The Feet
Overview
Pronation is the way the foot rolls inward when you walk and run. It is part of the natural movement that helps the lower leg deal with shock. Some people pronate more (overpronation) or less (underpronation) than others. Though this is not bad in itself, it does affect the way you run and it may increase the likelihood of injury. This makes your pronation pattern an important factor in choosing the right shoes.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
Wear shoes with straight or semicurved lasts. Motion-control or stability shoes with firm, multidensity midsoles and external control features that limit pronation are best. Over-the-counter orthotics or arch supports can help, too. You know you are making improvements when the wear pattern on your shoes becomes more normal. Overpronation causes extra stress and tightness to the muscles, so do a little extra stretching.
Prevention
Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips.
Pronation is the way the foot rolls inward when you walk and run. It is part of the natural movement that helps the lower leg deal with shock. Some people pronate more (overpronation) or less (underpronation) than others. Though this is not bad in itself, it does affect the way you run and it may increase the likelihood of injury. This makes your pronation pattern an important factor in choosing the right shoes.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
Wear shoes with straight or semicurved lasts. Motion-control or stability shoes with firm, multidensity midsoles and external control features that limit pronation are best. Over-the-counter orthotics or arch supports can help, too. You know you are making improvements when the wear pattern on your shoes becomes more normal. Overpronation causes extra stress and tightness to the muscles, so do a little extra stretching.
Prevention
Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips.
Bunions Cause And Effect
Overview
 A bunion is a bone deformity caused by an enlargement of the joint at the base and side of the big toe ( metatarsophalangeal joint ). Bunions form when the toe moves out of place. The enlargement and its protuberance cause friction and pressure as they rub against footwear. The growing enlargement or protuberance then causes more irritation or inflammation. In some cases, the big toe moves toward the second toe and rotates or twists, which is known as Hallux Abducto Valgus. Bunions can also lead to other toe deformities, such as hammertoe.
A bunion is a bone deformity caused by an enlargement of the joint at the base and side of the big toe ( metatarsophalangeal joint ). Bunions form when the toe moves out of place. The enlargement and its protuberance cause friction and pressure as they rub against footwear. The growing enlargement or protuberance then causes more irritation or inflammation. In some cases, the big toe moves toward the second toe and rotates or twists, which is known as Hallux Abducto Valgus. Bunions can also lead to other toe deformities, such as hammertoe.
Causes
With prolonged wearing of constraining footwear your toes will adapt to the new position and lead to the deformity we know as a foot bunion. Footwear is not the only cause of a bunion. Injuries to the foot can also be a factor in developing a bunion. Poor foot arch control leading to flat feet or foot overpronation does make you biomechanically susceptible to foot bunions. A family history of bunions also increases your likelihood of developing bunions. Many people who have a bunion have a combination of factors that makes them susceptible to having this condition. For example, if you are a women over the age of forty with a family history of bunions, and often wear high-heeled shoes, you would be considered highly likely to develop a bunion.
Symptoms
The dominant symptom of a bunion is a big bulging bump on the inside of the base of the big toe. Other symptoms include swelling, soreness and redness around the big toe joint, a tough callus at the bottom of the big toe and persistent or intermittent pain.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
Detecting and treating bunions can relieve many of the symptoms associated with this condition. Doctors often consider whether the condition requires non-surgical or surgical treatment. The decision is based on the severity of the symptoms. Because bunions often get worse over time, early detection and proper treatment are very important. Some non-surgical methods to reduce the symptoms related to bunions include cushioning the area with padding or tape, taking medication to relieve pain and inflammation, using physiotherapy to reduce pain and related symptoms (e.g., ultrasound, whirlpool baths, joint mobilization), wearing custom orthotics to provide better movement and stability of the foot, wearing well-fitted comfortable shoes that are not too tight (if your shoes used to fit but now are too tight around the bunion area, you may be able to have them stretched in this area), using a special splint at night to decrease the amount the toe angles towards the other toes. When non-surgical methods do not provide relief, surgery may be needed. During surgery, the doctor will remove the tissue or bone in the area of the bunion and attempt to straighten the big toe, and may join the bones of the affected joint. 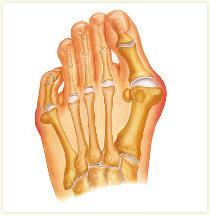
Surgical Treatment
Bunion surgery is occasionally required when the bunion deformity is too advanced for conservative treatment to work. Your surgeon will usually cut an angular section from the bone to correct the alignment. In some cases, multiple toes may need to be straighten.
Prevention
Here are some tips to help you prevent bunions. Wear shoes that fit well. Use custom orthotic devices. Avoid shoes with small toe boxes and high heels. Exercise daily to keep the muscles of your feet and legs strong and healthy. Follow your doctor?s treatment and recovery instructions thoroughly. Unfortunately, if you suffer from bunions due to genetics, there may be nothing you can do to prevent them from occurring. Talk with your doctor about additional prevention steps you can take, especially if you are prone to them.
Will Severs Disease Require Surgical Treatment?
Overview
Sever's disease, or calcaneal apophysitis, is a common cause of heel pain among active children between 10 to 13 years old. This spontaneous heel pain results from injury to the heel bone?s growth plate which is caused by overuse rather than specific injury or trauma. The condition is common among athletic children, particularly those active in soccer, football, and baseball. Treatment is available to reduce pain and discomfort associated with Sever's disease, but the condition usually resolves on its own once feet stop growing.
Causes
There are usually two root causes of Sever?s disease that we?ve found that effect young athletes. Arches are not supported causing a dysfunctional run, jump, and landing. The calves (gastrocnemius and soleus muscles) are overworked, tight, and do not allow proper movement of foot which puts extreme pressure on the Achilles? tendon, in turn irritating the growth plate in the heel.
Symptoms
The symptoms of Sever?s disease occur in the heel and the foot, and may worsen with activity. Pain and stiffness can occur in one or both heels. Symptoms can include. Swelling in the heel. Redness in the heel. Antalgic gait (such as limping). Foot pain or stiffness first thing in the morning or while walking. Pain that is worsened by squeezing the heel.
Diagnosis
Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage.
Non Surgical Treatment
Although most cases do get better on their own, recovery typically takes several weeks or months. Adolescents can continue to play sports if the activity does not cause discomfort, but staying active does prolong the recovery period without treatment. As a result, rest and avoidance of athletic activity is usually recommended, along with medication for pain and swelling.
Prevention
Treat symptoms when they occur with RICE and NO HARM. RICE (Rest Ice, Compression and Elevation) will help following activity and when symptoms flare, while No HARM (No Heat, alcohol, running or massage) will help reduce the symptoms from occurring. Orthotics. The use of an Interpod Orthotic will assist in realigning the foot, which will reduce the stress on the Achilles Tendon and prevent reoccurring symptoms. The orthotic achieves this by reducing the forces and stress placed on the limbs during walking and running. Exercise reduction. Patients may need to reduce their level of activity if this is seen as a contributing factor. Training errors. Ensue athletes warm up and cool down correctly with stretching activities. Footwear. Sporting and school shoes should have an appropriate heel height to assist in offloading of the Achilles tendon.
Sever's disease, or calcaneal apophysitis, is a common cause of heel pain among active children between 10 to 13 years old. This spontaneous heel pain results from injury to the heel bone?s growth plate which is caused by overuse rather than specific injury or trauma. The condition is common among athletic children, particularly those active in soccer, football, and baseball. Treatment is available to reduce pain and discomfort associated with Sever's disease, but the condition usually resolves on its own once feet stop growing.
Causes
There are usually two root causes of Sever?s disease that we?ve found that effect young athletes. Arches are not supported causing a dysfunctional run, jump, and landing. The calves (gastrocnemius and soleus muscles) are overworked, tight, and do not allow proper movement of foot which puts extreme pressure on the Achilles? tendon, in turn irritating the growth plate in the heel.
Symptoms
The symptoms of Sever?s disease occur in the heel and the foot, and may worsen with activity. Pain and stiffness can occur in one or both heels. Symptoms can include. Swelling in the heel. Redness in the heel. Antalgic gait (such as limping). Foot pain or stiffness first thing in the morning or while walking. Pain that is worsened by squeezing the heel.
Diagnosis
Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage.
Non Surgical Treatment
Although most cases do get better on their own, recovery typically takes several weeks or months. Adolescents can continue to play sports if the activity does not cause discomfort, but staying active does prolong the recovery period without treatment. As a result, rest and avoidance of athletic activity is usually recommended, along with medication for pain and swelling.
Prevention
Treat symptoms when they occur with RICE and NO HARM. RICE (Rest Ice, Compression and Elevation) will help following activity and when symptoms flare, while No HARM (No Heat, alcohol, running or massage) will help reduce the symptoms from occurring. Orthotics. The use of an Interpod Orthotic will assist in realigning the foot, which will reduce the stress on the Achilles Tendon and prevent reoccurring symptoms. The orthotic achieves this by reducing the forces and stress placed on the limbs during walking and running. Exercise reduction. Patients may need to reduce their level of activity if this is seen as a contributing factor. Training errors. Ensue athletes warm up and cool down correctly with stretching activities. Footwear. Sporting and school shoes should have an appropriate heel height to assist in offloading of the Achilles tendon.
The Facts Not Misconceptions About Ruptured Achilles Tendons
Overview
 A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon. Achilles tendon rupture occurs in people that engage in strenuous activity, who are usually sedentary and have weakened tendons, or in people who have had previous chronic injury to their Achilles tendons. Previous injury to the tendon can be caused by overuse, improper stretching habits, worn-out or improperly fitting shoes, or poor biomechanics (flat-feet). The risk of tendon rupture is also increased with the use of quinolone antibiotics (e.g. ciprofloxacin, Levaquin).
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon. Achilles tendon rupture occurs in people that engage in strenuous activity, who are usually sedentary and have weakened tendons, or in people who have had previous chronic injury to their Achilles tendons. Previous injury to the tendon can be caused by overuse, improper stretching habits, worn-out or improperly fitting shoes, or poor biomechanics (flat-feet). The risk of tendon rupture is also increased with the use of quinolone antibiotics (e.g. ciprofloxacin, Levaquin).
Causes
A rupture occurs when a patient overstretches the Achilles tendon, an act which causes it to tear partially or completely. Achilles tendon ruptures can occur during athletic play or any time the tendon is stretched in an unexpected way.
Symptoms
If your Achilles tendon is ruptured you will experience severe pain in the back of your leg, swelling, stiffness, and difficulty to stand on tiptoe and push the leg when walking. A popping or snapping sound is heard when the injury occurs. You may also feel a gap or depression in the tendon, just above heel bone.
Diagnosis
Your doctor will ask you about your symptoms and examine you. He or she may also ask you about your medical history. Your doctor may ask you to do a series of movements or exercises to see how well you can move your lower leg. He or she may also examine your leg, heel and ankle and may squeeze your calf muscle to check the movement of your foot. You may need to have further tests to confirm if your tendon is torn, which may include the following. An ultrasound scan. This uses sound waves to produce an image of the inside of your leg. An MRI scan. This uses magnets and radio waves to produce images of the inside of your leg.
Non Surgical Treatment
The best treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel; this allows the ends of your torn tendon to heal. This method can be effective, and it avoids the risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult. 
Surgical Treatment
The patient is positioned prone after administration of either general or regional anesthesia. A longitudinal incision is made on either the medial or lateral aspect of the tendon. If a lateral incision is chosen care must be taken to identify and protect the sural nerve. Length of the incision averages 3 to 10 cm. Once the paratenon is incised longitudinally, the tendon ends are easily identifies. These are then re-approximated with either a Bunnell or Kessler or Krackow type suture technique with nonabsorbable suture. Next, the epitenon is repaired with a cross stitch technique. The paratenon should be repaired if it will be useful to prevent adhesions. Finally, a meticulous skin closure will limit wound complications. An alternative method is to perform a percutaneous technique, with a small incision (ranging from 2-4 cm). A few salient points include: the incision should be extended as needed, no self-retaining retractors should be used, and meticulous paratenon and wound closure is essential. Postoperatively the patient is immobilized in an equinous splint (usually 10?-15?) for 2 weeks. Immobilization may be extended if there is any concern about wound healing. At the 2-week follow-up, full weight bearing is permitted using a solid removable boot. At 6 weeks, aggressive physical therapy is prescribed and the patient uses the boot only for outdoor activity. At 12 weeks postoperatively, no further orthosis is recommended.
Leg Length Discrepancy Lifts
Overview
A Leg Length Inequality or Leg Length Discrepancy is exactly as it sounds. One or more bones (the Femur or thigh bone, the Tibia or shin bone, and/or the joint spacing within the knee) are unequal in total length when measured in comparison to the same structures on the opposite side. It is common for people to have one leg longer than the other. In fact, it is more typical to be asymmetrical than it is to be symmetrical.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
The most common symptom of all forms of LLD is chronic backache. In structural LLD the sufferer may also experience arthritis within the knee and hip are, flank pain, plantar fasciitis and metatarsalgia all on the side that is longer. Functional LLD sufferers will see similar conditions on the shorter side.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.

Surgical Treatment
Surgery to shorten the longer leg. This is less involved than lengthening the shorter leg. Shortening may be done in one of two ways. Closing the growth plate of the long leg 2-3 years before growth ends (around age 11-13), letting the short leg catch up. This procedure is called an epiphysiodesis. Taking some bone from the longer leg once growth is complete to even out leg lengths. Surgery to lengthen the shorter leg. This surgery is more involved than surgery to shorten a leg. During this surgery, cuts are made in the leg bone. An external metal frame and bar are attached to the leg bone. This frame and bar slowly pull on the leg bone, lengthening it. The frame and bar must be worn constantly for months to years. When the frame and bar are removed, a leg cast is required for several months. This surgery requires careful and continued follow-up with the surgeon to be sure that healing is going well.
A Leg Length Inequality or Leg Length Discrepancy is exactly as it sounds. One or more bones (the Femur or thigh bone, the Tibia or shin bone, and/or the joint spacing within the knee) are unequal in total length when measured in comparison to the same structures on the opposite side. It is common for people to have one leg longer than the other. In fact, it is more typical to be asymmetrical than it is to be symmetrical.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
The most common symptom of all forms of LLD is chronic backache. In structural LLD the sufferer may also experience arthritis within the knee and hip are, flank pain, plantar fasciitis and metatarsalgia all on the side that is longer. Functional LLD sufferers will see similar conditions on the shorter side.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.
Surgical Treatment
Surgery to shorten the longer leg. This is less involved than lengthening the shorter leg. Shortening may be done in one of two ways. Closing the growth plate of the long leg 2-3 years before growth ends (around age 11-13), letting the short leg catch up. This procedure is called an epiphysiodesis. Taking some bone from the longer leg once growth is complete to even out leg lengths. Surgery to lengthen the shorter leg. This surgery is more involved than surgery to shorten a leg. During this surgery, cuts are made in the leg bone. An external metal frame and bar are attached to the leg bone. This frame and bar slowly pull on the leg bone, lengthening it. The frame and bar must be worn constantly for months to years. When the frame and bar are removed, a leg cast is required for several months. This surgery requires careful and continued follow-up with the surgeon to be sure that healing is going well.